For the last 16 years, Dr. Josiah Rich has gone weekly to prisons in or near Providence, R.I., to treat people being held there for drug-related offenses. Each time, he has wrestled with an ethical conundrum: not the issue of whether the offenders have done something wrong, but whether the American prison system is doing something worse. "What I see is not bad people," he says. "Predominantly, I see people with a disease."
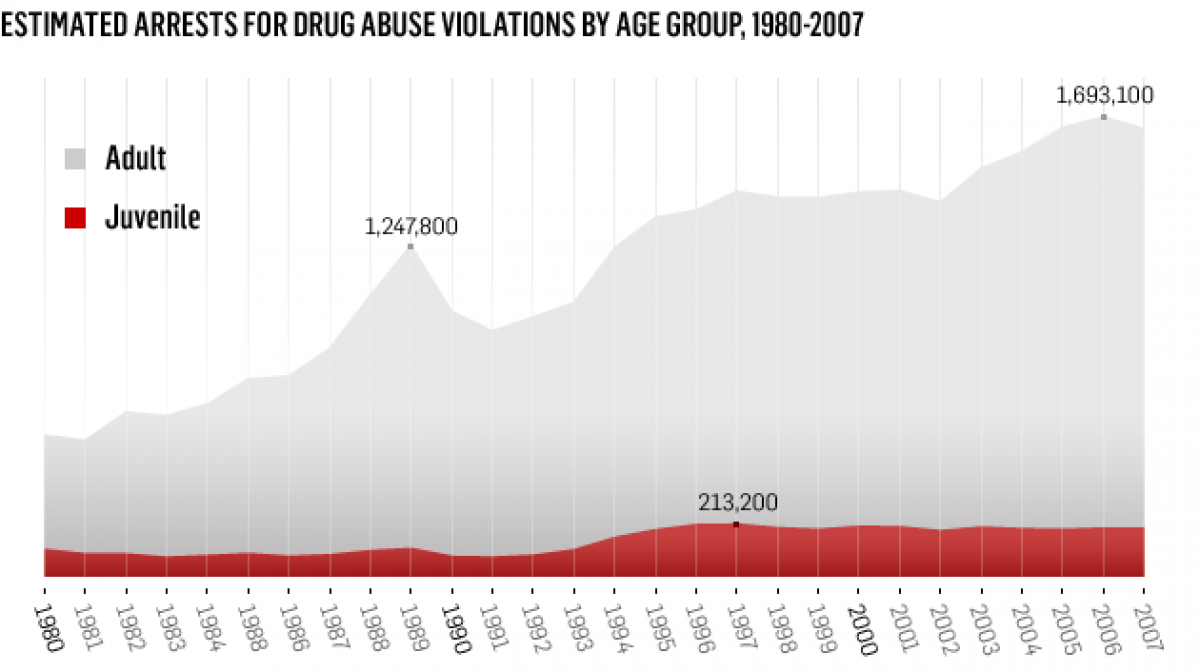
Of the 2.3 million inmates in the U.S., more than half have a history of substance abuse and addiction. Not all those inmates are imprisoned on drug-related charges (although drug arrests have been rising steadily since the early 1990s; there were 195,700 arrests in 2007). But in many cases, their crimes, such as burglary, have been committed in the service of feeding their addictions. Rich, a professor of medicine and community health at Brown University, is worried that, by refusing or neglecting to provide treatment to these addicts, many U.S. prisons are missing the best chance to cure them—and in the process to cut down on future crime. Treatment can reduce recidivism rates from 50 percent to something more like 20 percent, according to the DEA. Yet it is not widely provided. "Our system has taken the highest-risk and most ill people and put them in a place where they have constitutionally mandated health care," Rich says. "What a great opportunity to make a difference. Are we just trying to punish people? Or are we trying to rehabilitate people? What do we want out of this?"
Looking at the way prisons currently deal with drug addiction, the answer to Rich's question is unclear. Over the last few years, some in the justice system have warmed to the idea of treating drug addicts in addition to (or instead of) incarcerating them. In some states, most notably Ohio, almost all first-time drug offenders and many second-timers are offered treatment. That is by no means the case nationally. According to a report released last year by the National Institute on Drug Abuse, just one fifth of inmates get some form of treatment. That number may be lower in the near future: tight budgets are forcing many states to cut back or close down their existing treatment programs. Kansas and Pennsylvania have already done so; California and Texas may follow suit in the next few months.
The irony here is that by lowering recidivism, the programs themselves save money in the long run. The NIDA report released last year cited a remarkable statistic: heroin addicts who received no treatment in jail were seven times as likely as treated inmates to become re-addicted, and three times as likely to end up in prison again. For every dollar spent, the programs save $2 to $6 by reducing the costs of re-incarceration, according to Human Rights Watch. Looked at another way, the programs can save the justice system about $47,000 per inmate.
So why would prisons target their own treatment programs in an effort to cut costs? Part of the reason is that pharmacological treatment—such as giving heroin addicts methadone to help them through withdrawal—requires a lot of regulation, and thus it's expensive in the short run. Pharmacological treatment isn't the only way of helping addicts—the White House's drug-policy arm has a good list of other options—but in many cases it's the most effective. Unfortunately, it's also very tricky. It can be undermined by the fact that addicts can easily relapse behind bars; a Human Rights Watch report last year claimed that "drugs are as available in prison as in the street," often getting to inmates via the mail. (Reliable statistics on inmate drug use are understandably hard to come by, since prisoners have no reason to fess up to using.) There are other challenges, too, particularly in treating addicts with methadone. "People are loath to provide methadone because it poses some security risk," says Dr. Amy Nunn, also a professor of medicine at Brown. "It could be diverted or sold on the black market, or someone might rob the dispensary." When methadone is given, it's usually with strict oversight at a medical center, not as a matter of course in the correctional facility. That takes money. Buprenorphine, which is used to treat opioid addicts, is a little easier for prisons to deal with because it's "harder to divert," Nunn adds. The medication has an additive that prevents it from being crushed up and inhaled. But it is not widely used either. Only half of all states and prisons provide any form of methadone or buprenorphine treatment, and those that do make use of the drugs do so in a limited fashion, even though the WHO has both medications on a list of drugs that should be available to all prisoners at any time.
But Nunn says the real problem is an ideological one, not a practical one. "In spite of all of the proven clinical and social and economic benefits of pharmacological treatment, people really have a moral opposition to it," she says. "They think if you're providing people with treatment, you're not addressing their addiction in an appropriate way. They think people who have addictions deserve what they get, and that the only way to treat addiction is abstinence, when nothing could be further from the truth."
Steven Belenko, a professor of criminal justice at Temple University, adds that people who work in prisons don't necessarily think that way: "Correctional professionals recognize the importance of these types of services," he says. Bob May, associate director of the Association of State Correctional Administrators, agrees. He says people who work in the system "acknowledge the value of the programs. There was a time, years ago, when that wasn't the case. People weren't convinced that the programs were effective, or even cost-effective. When I was working as chief of detectives in a sheriff's department, I didn't believe in these programs, either. My job was to put people away. You know, you think it's just some bleeding-heart liberal trying to make excuses for a crime. But I didn't know that 75 to 80 percent of people I was arresting for other crimes had an abuse problem." Now, he adds, "we know from the research that with people who go through drug treatment, even if they still use drugs afterwards, their crimes are less violent and less frequent. Even if it's not a 100 percent change, it's a good thing." The public doesn't necessarily think treatment is bad, either; a recent poll found that more than two thirds of Americans would support state laws requiring treatment—not jail time—for first- and second-time drug offenders.
But politicians may oppose treatment (at least publicly), especially if they're worried about being seen as soft on crime. And even if they support the idea, with state budgets under a crunch, treatment can start to look expendable. "It's the legislators who are funding or not funding these types of things," Belenko says. "So even when prison systems are very open and supportive of treatment, they face a bunch of administrative constraints and cost constraints. They don't have enough funds to do this."

That's been the case as long as treatment programs have been around, judging by a 1991 government report, which showed that only a fifth of drug-addicted inmates who needed treatment were able to get it. But the current economy has made things worse. In Florida, for instance, corrections secretary Walter McNeil recently suggested—"reluctantly," according to the St. Petersburg Times—a $36 million budget cut that would close "most of the state's publicly funded treatment centers."
Then there's Texas. In 2003 the state government (largely led by Republicans) started to whittle away at treatment programs. Four years later, thanks to efforts led by State Sen. John Whitmire, it changed course, putting more money into them, rather than less, and adding 6,000 "beds" available to treat nonviolent prisoners who have substance-abuse issues. Whitmire, who had been robbed at gunpoint by a cocaine addict, says that sometimes convincing fellow legislators of the value of more treatment was a "hard sell," but he told them this was a public-safety issue: "I've begged for my life once from someone addicted to cocaine," he says. "I would much rather spend money on his addiction than face that gun again. This isn't about being soft on crime. It's about being tough, but also smart."
His initiative saw positive results initially: the prison population, predicted to climb by more than 5,000 by the end of 2008, grew by only a 10th of that. Public and political opinion, even among Republicans, started to turn in favor of treatment—until earlier this year, when Gov. Rick Perry asked each state agency to slash 5 percent from their budgets. Once again, treatment ended up on the chopping block. The Texas Department of Criminal Justice proposed to slash $23 million from treatment programs. Whitmire argued successfully against that proposal, but now the system faces an even larger pending cut of 10 percent.
According to a report commissioned by the Justice Center at the Council of State Governments, "Of the proposed $124.3 million FY 2010–11 reduction [in Texas], $109.4 million, or 88 percent, will be reductions in probation and parole supervision, alternatives to incarceration, mental health services, substance abuse treatment, halfway houses, and intermediate sanction facilities." Tony Fabelo, director of research at the CSG and a coauthor of the report, says "the only way to save money," at least in the short term, "is shutting down programs or shutting down prisons. And if there were an outcry about shutting down programs, there would be a bigger one about shutting down prisons. So those are the dynamics where we are trapped."

That is deeply concerning to Whitmire. "If we do not continue these programs, people will re-offend, recidivism rates will rise, and it will be a danger to the public," he says. "You either pay now, or pay later—and you pay a lot more later."
What happens to addicts who don't get treatment in prison? Often they return to their addiction upon their release. "When somebody's addicted to heroin and they don't get treatment, they're [likely] to get addicted to heroin again," says Rich. "The drug has biologically changed their brains. You can tie someone down and make sure they don't use any opiates and you can keep them there for years, and the day they walk out, they [can] get opiates."
And then they're likely to wind up back in the prison system. That's bad news for the inmates, the prisons, and the taxpayers, since, as Rich puts it, treatment is "certainly cheaper than the gobs of money we're spending to keep locking people up."
In other words, no matter how you feel about drug-addicted inmates, you're going to pay for dealing with their addiction. So why aren't we choosing the cheaper—and arguably more humane—option?
Find out more about the social and economic impact of America's prisons in our series. Read about the debate over whether cash-strapped states should cut classrooms or prison cells, and find out how the recession is slamming private jails.
Uncommon Knowledge
Newsweek is committed to challenging conventional wisdom and finding connections in the search for common ground.
Newsweek is committed to challenging conventional wisdom and finding connections in the search for common ground.
About the writer
To read how Newsweek uses AI as a newsroom tool, Click here.